|
How Menstruation
Actually Occurs (at the Microscopic Level) Nelson
Soucasaux |
 |
First, lets us describe some basic aspects of the endometrial histology and physiology.
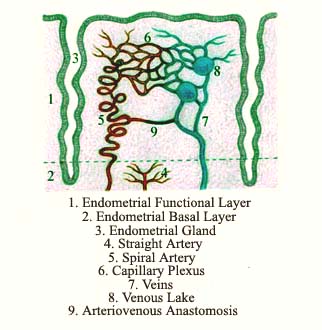
As widely known, two layers can be distinguished in the endometrium ( the uterine inner lining ): the functional and the basal. The endometrial functional layer is the one that is entirely expelled and reconstructed at each menstrual cycle. When fully developed under the action of the ovarian hormones, it reaches considerable thickness. The endometrial functional layer is highly responsive to the estrogens' proliferative effect and to progesterone's secretory transformation. A highly complex system of spiral arteries, capillary networks and plexuses, veins, venous lakes and arteriovenous anastomosis constitutes its blood supply. Of all structures that integrate this vascular system, the spiral arteries are the most important ones. Actually, we may say that what makes the occurrence of menstruation possible are just these spiral arteries.
As the blood
levels of the ovarian hormones fall, the endometrial functional layer
immediately undergoes regression, shrinkage and atrophy. This causes the
formation of toxic and vasoactive substances which, by local action, trigger
the ischemic and hemorrhagic phenomena that finally results in the necrosis
and desquamation of this endometrial layer. Menstruation just happens
as a consequence of the very peculiar way through which the endometrial
vascular system reacts to the regressive changes that result from the
sudden fall of the ovarian hormones ( as well as the sudden fall of administered
exogenous female hormones ).
The endometrial basal layer is rather thin and lies deeply, in
direct contact with the myometrium. As it does not desquamate during
menstruation, this layer provides the histologic elements from which
a new functional layer develops when the menstrual bleeding ceases. The
basal layer is much less responsive to the hormonal stimuli and its blood
supply is due to another vascular system, constituted by small straight
arteries. In this way, it does not undergo the necrotic, ischemic and
hemorrhagic phenomena of the menstrual period and, for that reason, is
always preserved.
Menstruation depends on two factors, an endocrine and a vascular. The endocrine one is the sudden fall in the blood levels of the ovarian hormones and is the main menstrual triggering factor. The vascular reactions constitute a very peculiar and unique phenomenon resulting from the involutive endometrial changes caused by the sudden hormonal fall. The intimate mechanisms of menstruation lie just here, at the vascular level. So, let us finally go to a more detailed description of these very curious endometrial vascular patterns that constitute the main subject of this article.
The arteries that cross the uterine walls and are responsible both for the myometrial and the endometrial blood supply are named radial arteries. As their minor branches arrive close to the myometrial-endometrial junction, they give rise to the aforementioned spiral and straight arteries, which penetrate into the endometrium through its basal layer.
The straight arteries are very short and small and, as already said, provide the blood supply only and exclusively to the endometrial basal layer. Their division into smaller arterioles, capillary and venous networks follows the same pattern of almost all other tissues in the body.
On the other hand, the spiral arteries, which are highly sensitive to the estrogens and progesterone, penetrate the endometrial functional layer, grow and send branches within it and exhibit very different and unique patterns. One of the reasons that account for this is that, along the cycle, these arteries grow much faster than the rest of the endometrial functional layer. Though both the functional layer and its blood supply ( provided mostly by these spiral arteries ) develop together at each menstrual cycle, the growth of each one of them takes place at a different rate.
This means that the spiral arteries grow in length much faster than the whole endometrium grows in thickness. So, considering this great lengthening of the spiral arteries, as the endometrium develops and presents several changes along the cycle, these arteries have to "accommodate" inside it by continuously accentuating their coiling. At the same time, this progressive coiling of the spiral arteries also plays a very important function in the endometrial physiology : it triggers the vascular mechanisms of menstruation.
In 1954, F.H. Netter had already observed that this pattern, "... unique to the endometrium, is believed to be the mainspring of the process which enacts the rhythmic necrosis and hemorrhage called menstruation, although the parts played by individual vessels before and during the bleeding period are not altogether clear" ( see Note below ).
The spiral arteries give rise to two types of smaller arterial branches: 1) the common ones ( similar to all others in the body ), which originate the usual arteriovenous capillary plexuses and networks that nourish all the functional endometrial layer; 2) arteriovenous anastomosis, through which branches of the spiral arteries merge directly into the endometrial veins, constituting a kind of vascular "shunt", without any previous division into capillaries. As to the endometrial veins, they are not spiraled but exhibit many dilations named "venous lakes."
As already said, as the sudden fall in the blood levels of the ovarian hormones takes place at the end of the cycle, the functional endometrial layer immediately exhibits signs of involution, shrinkage and atrophy. This endometrial shrinkage, in turn, "forces" the spiral arteries to coil more and more, and this excessive coiling ends up by restricting the normal blood flow to the endometrial functional layer. This reduction in the blood flow associated with the endometrial involution, shrinkage and atrophy accelerates the process of necrosis of that tissue. Netter had also remarked that, as the endometrium shrinks, it "... becomes more dense and forces therewith the spiral arteries to kink and 'buckle.' A slowed-down circulation, or even stasis, ensues..." ( Note below ).
The beginning of the necrotic process, in turn, seems to give rise to the production of toxic and vasoactive substances that cause an intense vasoconstriction in the spiral arteries, finally resulting in severe endometrial ischemia and the complete necrosis of its functional layer. In the recent past, some authors used to refer to this process as a kind of physiological endometrial "infarction."
Due to the spiral arteries' vasoconstriction, most of their blood flow abruptly goes through the arteriovenous anastomosis directly to the endometrial veins and venous lakes ( these anastomosis actually form alternative vascular circuits ). As most of the endometrium is already necrotic due to the ischemia and other degenerative processes due to the hormonal sudden fall, there is a rupture not only of the venous lakes but also of the capillary system, resulting in an hemorrhage that quickly spreads through the entire endometrial functional layer. In this way, first there is an endometrial ischemia which, immediately afterwards, is followed by the endometrial hemorrhage. The hemorrhage, together with the uterine contractions stimulated by the increased production of prostaglandins resulting from the endometrial involution, helps the uterus to eliminate the necrotic functional layer of the endometrium, promoting a periodic renewal of this tissue. So, at the small details of this very peculiar and unique endometrial blood supply, that's basically how that physiological uterine bleeding named menstruation takes place...
Note:
Netter, F.H. - "The Ciba Collection of Medical Illustrations -
Volume 2, Reproductive System" - USA, 1954.
P.S.:
The anatomical drawing was adapted and modified from a Netter's original
by Nelson Soucasaux.
![]()
Nelson Soucasaux
is a gynecologist dedicated to Clinical, Preventive and Psychosomatic
Gynecology. Graduated in 1974 by Faculdade de Medicina da Universidade
Federal do Rio de Janeiro, he is the author of several articles published
in medical journals and of the books "Novas
Perspectivas em Ginecologia" ("New Perspectives in Gynecology")
and "Os Órgãos Sexuais Femininos:
Forma, Função, Símbolo e Arquétipo" ("The
Female Sexual Organs: Shape, Function, Symbol and Archetype"),
published by Imago Editora, Rio de Janeiro, 1990, 1993.
![]()
![]()
[ Home
] [ Consultório (Medical Office)
] [ Obras Publicadas (Published Works)
]
[ Novas
Perspectivas em Ginecologia (New Perspectives in Gynecology)
]
[ Órgãos Sexuais Femininos (The
Female Sexual Organs) ]
[ Temas
Polêmicos (Polemical Subjects) ] [ Tópicos
Diversos (Other Topics) (Part 1) ]
[ Tópicos
Diversos (Other Topics) (Part 2) ] [ Tópicos
Diversos (Other Topics) (Part 3) ]
[ Tópicos
Diversos (Other Topics) (Part 4) ] [ Tópicos
Diversos (Other Topics) (Part 5) ]
[ Ilustrações (Illustrations)
]
Email: nelsons@nelsonginecologia.med.br
![]()